Every story has a beginning. This one starts in late 2001, when my father-in-law fractured three of his ribs. Harry was a retired physician, and after a thorough workup that he insisted on, it turned out that his bone density was severely compromised for no immediately apparent reason. Further tests eventually revealed the cause: He had multiple myeloma, a cancer of the bone marrow.
Harry’s cancer was caught early, and it progressed slowly. By 2007, however, it had taken over his body. When my wife saw him in early 2008, she remarked that he looked like someone in a lot of pain but trying not to show it—despite the fact that he was taking oxycodone, a powerful opiate.
During a career that lasted more than three decades, he had watched all too many of his patients struggle with their final months, and this experience had persuaded him that he would take his own life if he found himself dying of an agonizing and clearly terminal illness. Now he was. Finally, on the evening of January 29, he stumbled and fell during the night, and decided his time had come: He was afraid if he delayed any longer he’d become physically unable to remain in control of his own destiny.

This was important. Since Harry lived in California, where assisted suicide was illegal, he had to be able to take his life without help. Because of this, he initially intended not to tell either of his daughters about his decision. He wanted to run absolutely no risk that merely by being with him in his final moments, or even knowing of his plans, they’d be held responsible for his death.
Luckily, neither my wife nor her sister had to learn of their father’s death via a call from the morgue. A friend persuaded him to call both of them, and on January 30 we all drove out to Palm Springs to say our last goodbyes. After that, Harry wrote a note explaining that he was about to take his own life and that no one else had provided any assistance. It was time. He categorically forbade any of us from so much as taking his arm. He walked into his bedroom, put a plastic bag over his head, and opened up a tank of helium. A few minutes later he was dead.
Why helium? Why the note?
Harry was a methodical man, and when he decided he would eventually take his own life, he naturally looked for advice. The place he turned to was the Hemlock Society, founded in 1980 with a mission of fighting to legalize physician-assisted suicide for terminally ill adults.
When we went through Harry’s files after his death, we found a slim manila folder with several pages copied from various Hemlock publications, nestled between a bunch of fat folders containing financial information, his will, and his medical records. One of the pages recommended that you write a note making it clear that you had taken your own life, unassisted by anyone else. This was meant for the sheriff or the coroner, and was designed to protect anyone who might be suspected of illegally aiding you.
There were also several pages with instructions on how to take your life using an “inert gas hood kit.” This is a fairly simple and painless way to die, since your body reflexively wants to breathe, but doesn’t really care what it breathes. If you breathe pure helium, or any other inert gas, you won’t feel any sensation of suffocation at all. You simply fall unconscious after a minute or so, and within a few more minutes, you die.
At the time of Harry’s death, the Hemlock Society—known today as Compassion & Choices—was one of the oldest and best-known organizations working to legalize physician-assisted suicide. But it was hardly the first. During the 19th century, as opioid painkillers became widespread, euthanasia became a lively topic of discussion. By the turn of the century it had been banned in nearly every state. Public opinion finally started to shift in the 1930s, and by 1949 it had progressed enough that the Euthanasia Society of America was able to recruit several hundred Protestant and Jewish clergymen in an effort to challenge New York’s law prohibiting physician-assisted suicide. Thanks partly to fresh memories of the infamous Nazi “forced euthanasia” programs that killed thousands of the disabled and mentally ill, and partly to the Catholic Church’s opposition to any form of suicide, their effort failed.
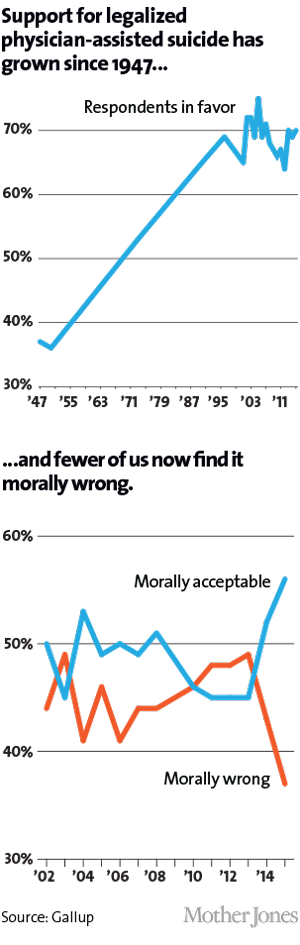
Still, support for physician-assisted suicide continued to tick slowly upward, from 37 percent in 1947 to 53 percent by the early ’70s, when the birth of the patients’ rights movement helped shine a new spotlight on issues of death and dying. Karen Ann Quinlan provided the spark when she fell into a coma and was declared by doctors to be in a “persistent vegetative state.” Her parents went to court to have her respirator removed, and in 1976 the New Jersey Supreme Court ruled in their favor. That year California became the first state to recognize living wills as legally binding documents that authorize the removal of life-sustaining treatment in the face of imminent death. Other states followed, and end-of-life directives became an increasingly common part of the medical landscape. Today, there’s hardly a medical show on television that hasn’t dealt with the now-famous DNR—Do Not Resuscitate—order.
Active euthanasia remained illegal everywhere, but the door had been opened a crack—and supporters of assisted suicide started pushing to open it further. Founded in the aftermath of the Quinlan fight, the Santa Monica-based Hemlock Society soon became one of the most aggressive backers of abolishing legal bans on physician-assisted suicide. By the end of the 1980s, national support had gained another 12 polling points, and success seemed within grasp. In 1988, supporters of assisted suicide tried but failed to get a measure on the California ballot. In 1991, a similar measure made it on the ballot in Washington state but failed to gain passage. In 1992, Californians got a measure on the ballot, and polls showed the public widely in favor. But a well-funded opposition campaign, led by the Catholic Church, took its toll, and in the end the initiative failed, 54 to 46 percent. Finally, in 1994, backers succeeded in Oregon. Three years later, following a court fight and a second ballot measure, Oregon became the first state to legalize physician-aided suicide.
Ever since Oregon’s Death With Dignity Act took effect in 1997, the state health authority has published annual reports about the numbers and types of patients who have gotten a prescription for DWDA drugs. Probably the main takeaway is the simplest one: If Oregon is any indication, assisted suicide will never be a popular option. In 1998, only 24 people received DWDA prescriptions, and 16 used them. By 2014, after 16 years in which Oregonians could get used to the idea, 155 people requested prescriptions, and 105 used them. That’s 105 out of about 34,000 total deaths statewide, or roughly one-third of 1 percent.
Part of this is due to the stringency of Oregon’s law. Requests for DWDA drugs must be confirmed by two witnesses and approved by two doctors. The patient must not be mentally ill. And most important of all, both doctors have to agree that the patient has no more than six months to live. Because of this, about two-thirds of all patients who requested drugs had cancer, an illness that frequently has a definite timeline. Only about one-sixth have degenerative diseases with indeterminate timelines, like Alzheimer’s or ALS—Lou Gehrig’s disease.
In the decade after Oregon’s law took effect, the physician-assisted-suicide movement gained little ground. On a national level approval rates remained steady, with about two-thirds of Americans telling Gallup they supported the concept, but that seemingly strong support didn’t translate into legislative success.
Some of the reasons for this failure are obvious, but among the obscure ones is this: Assisted suicide has long been a West Coast movement. During the late 1980s and early 1990s, California, Oregon, and Washington all had active legislative legalization campaigns—even if only Oregon’s succeeded—and according to a 1996 survey, West Coast doctors received many more requests for assisted suicide than doctors in other parts of the country. No one is quite sure why, but outside of the West Coast, it was simply not a very prominent issue.
Another reason legalization failed to gain ground is rooted in semantics. Miles Zaremski, an attorney who has argued on behalf of such bills for years, is typical of assisted-suicide supporters when he maintains that in the case of terminal patients, “we’re not dealing with the concept or notion of suicide at all.” Rather, it’s nothing more than aiding the natural dying process. Opponents call this Orwellian and worse. Public sensitivities reflect this linguistic divide. Although that longitudinal Gallup poll has long reported two-thirds support for legally allowing doctors to “end the patient’s life by some painless means,” support historically drops by 10 points or more when they ask if doctors should be allowed to “assist the patient to commit suicide.” So when legislation is under consideration, opponents fill the airwaves with the word “suicide,” and public support ebbs.
A third reason is demographic: The assisted-suicide movement has long been dominated by well-off, educated whites. As early as 1993, Dick Lehr reported in a Boston Globe series titled “Death and the Doctor’s Hand” that every doctor he talked to said that patients who asked about assistance in dying were typically middle to upper class and accustomed to being in charge. As one oncologist put it, “These are usually very intelligent people, in control of their life—white, executive, rich, always leaders of the pack, can’t be dependent on people a lot.”
In fact, one of the reasons Oregon was first to pass an assisted-suicide bill is likely because it’s a very white state—and so are the patients who take advantage of the Death With Dignity Act. The 2014 report from the Oregon Health Authority says that the median age of DWDA patients is 72 years old; 95 percent are white, and three-quarters have at least some college education.
Aid-in-dying bills are a tougher lift in more-diverse states. Minority patients have historically been wary of the medical establishment, and not without reason. There’s abundant evidence that people of color have less access to health care than whites and receive less treatment even when they do have access. If the health care system already shortchanges them during the prime of their lives, would it also shortchange them at the end, pressing them to forgo expensive end-of-life care and just take a pill instead? This fear makes the doctors who serve them cautious about discussing assisted suicide. “My concern is for Latinos and other minority groups that might get disproportionately counseled to opt for physician-assisted suicide,” one doctor told Lehr. More recently, Dr. Aaron Kheriaty, director of the medical ethics program at the University of California-Irvine School of Medicine, explained to the New York Times, “You’re seeing the push for assisted suicide from generally white, upper-middle-class people, who are least likely to be pressured. You’re not seeing support from the underinsured and economically marginalized. Those people want access to better health care.”
Finally, there’s the fourth and most obvious reason for legislative failures: Assisted suicide has a lot of moral opposition.
Suicide has always been a sin to the Catholic Church, and in 1965 the Vatican reaffirmed this position, declaring that abortion, euthanasia, and other forms of taking life “poison human society.” In 1980, the church released its “Declaration on Euthanasia,” which permitted the refusal of extraordinary measures when death was imminent but categorically opposed any kind of assisted suicide, calling it a “violation of the divine law.” In 1995, Pope John Paul II issued his Evangelium Vitae encyclical, which condemned the growing acceptance of euthanasia as a personal right.
It was Evangelium Vitae that popularized the epithet “culture of death,” which has since been adopted by born-again Christians to condemn both abortion and assisted suicide. This makes assisted-suicide legislation especially difficult to pass in states with a large Catholic or conservative Christian presence.
Opposition also comes from many within the disability rights movement, who have a long-standing wariness of the medical community. “Doctors used to exercise near-total control over the lives of people like me with significant disabilities,” writes Diane Coleman, a disability rights activist, “sentencing us to institutions, and imposing their own ideas about what medical procedures would improve our lives.” That attitude has since improved, but not enough to allay fears that doctors might care for the disabled differently if assisted suicide becomes legal. Will they treat depression in the disabled with less than their usual vigor, giving in more easily to requests for lethal drugs? Consciously or unconsciously, will they be more likely than they should be to diagnose imminent death?
And it’s not just doctors. The seriously disabled already live with the reality that many people consider their lives barely worth living in the first place. They fear that if assisted suicide becomes commonplace, the right to die could evolve into a “duty to die,” and those with disabilities—along with minorities and the poor—might face increased pressure to end their lives. The pressure could come from family members, exhausted from tending to disabled children or parents. It could come from insurance companies, for which assisted suicide is a lot cheaper than six months of expensive end-of-life care. It could come from government “death panels,” trying to control costs and keep taxes low. Or it could come from the disabled themselves, out of worry that they’re a burden on friends and family, both emotionally and financially.
More generally, opposition also comes from those who fear a slippery slope. In the Netherlands, where euthanasia is legal, 1 in 28 deaths now comes via doctor-assisted suicide. That’s up 200 percent in the past decade, largely because the rules are so lenient. All you have to do is claim unbearable suffering, which in practice can mean that you’re just tired of living.
Opposition also comes from the medical profession itself. This has softened over the past few years, with a large 2010 survey showing that more physicians supported assisted suicide (45 percent) than did not (40 percent). Nonetheless, until last year both the American Medical Association and every single state medical group formally opposed physician-aided suicide.
In California, all of these things—its large Latino population, its large Catholic population, the opposition of doctors, and real concerns about both slippery slopes and pressure on the poor—conspired for years to keep assisted suicide from becoming legal. In the past quarter century, advocates tried five times to pass legislation legalizing the practice—via ballot measures in 1988 and 1992 and legislation in 1995, 1999, and 2005. Five times they failed.
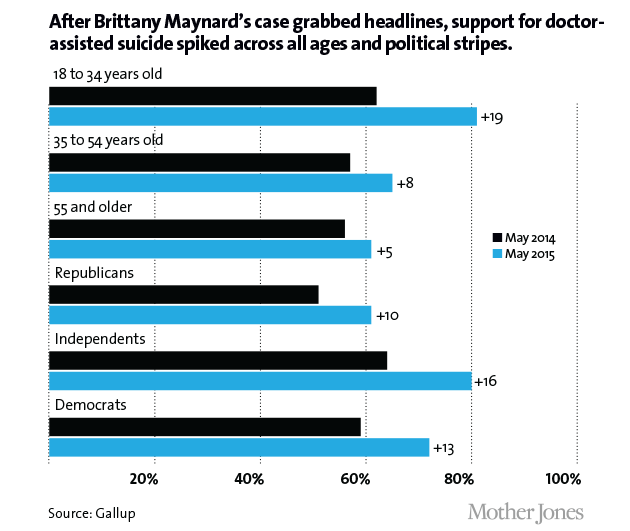
Then Brittany Maynard happened.
For California’s assisted-suicide movement, Brittany Maynard was perfect: young, attractive, articulate, dying of a brain tumor—and very much on their side. Marcia Angell, a former editor of the New England Journal of Medicine, called her “the new face of the movement.“
Maynard’s cancer was diagnosed on the first day of 2014. She underwent surgery to remove the tumor, but in April it returned, worse than ever. A few months later she moved from San Francisco to Oregon and partnered with Compassion & Choices—the successor to the Hemlock Society—to create a six-minute video explaining why she wanted the right to control the time and manner of her death. It has been viewed nearly 12 million times since then. In October, she was featured on the cover of People. On November 1, she took the pills she had been prescribed and died.
Maynard’s story galvanized the cause of assisted suicide in California. Two months after her death yet another bill was introduced. It passed the state Senate in June, but opposition from church leaders, disability rights activists, and others bottled it up in the Assembly’s Health Committee in July. Nationally, support for “assisted suicide” was up 17 points, and had finally hit the same two-thirds level in Gallup polls that “ending life painlessly” had long maintained. State polls showed even stronger support: Californians approved it by a margin of 71 to 22 percent. Nevertheless, for the sixth time, assisted suicide couldn’t quite find enough votes even to make it out of committee.
Then supporters got a lucky—and totally unexpected—break: Gov. Jerry Brown called for a special legislative session to address Medicaid funding issues. Unsurprisingly for California, those funding issues haven’t yet been resolved. But equally unsurprisingly, California legislators had no intention of letting a special session go to waste. Dozens of measures were brought up, and one of them was the assisted-suicide bill that had failed only a month earlier. This time, though, things were different. Special-session rules allowed supporters to exclude from the Health Committee five Democrats who had opposed it earlier in the year. With that, the bill finally made it to a floor vote.
It also helped that the bill had a list of safeguards even longer than Oregon’s. Patients must be competent adults with no diagnosed mental disorders that would impair judgment. Two doctors have to certify that patients have less than six months to live. Doctors are required to meet privately with patients to ensure they aren’t being coerced. Two oral requests for aid-in-dying drugs must be made 15 days apart, along with a written request. Only the attending physician can prescribe the medication. The drugs must be self-administered. And the law expires automatically in 10 years unless the Legislature reenacts it.
On September 9, ABX2-15 was passed by the Assembly. On September 11, it was passed by the state Senate. On October 5, after a month of silence about his intentions, Brown signed it into law. Sometime in 2016—90 days after the Legislature adjourns the special session—assisted suicide will finally be legal in California.
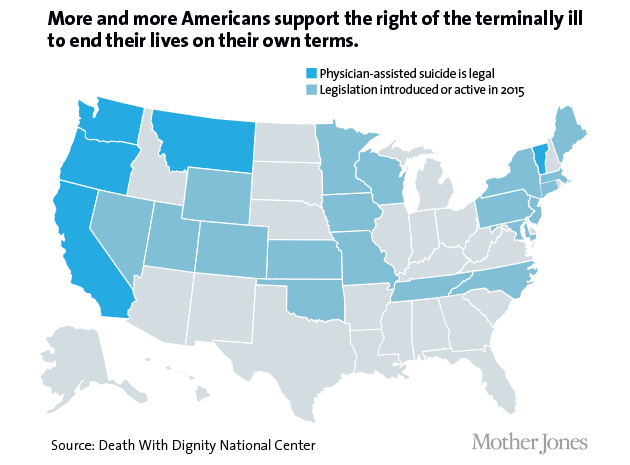
For more than a decade after Oregon passed the nation’s first assisted-suicide law, no other state followed. Then, in 2008, Washington voters passed a ballot measure legalizing the practice. In 2009, it was legalized by court order in Montana. Vermont’s lawmakers followed in 2013. Now, the addition of California has tripled the number of Americans with the right to ask a physician for a lethal prescription if they have a terminal disease.
Does this mean that assisted suicide is the next big civil rights battle? The fact that four states have approved assisted suicide in just the past seven years suggests momentum may finally be reaching critical mass. What’s more, if Gallup’s polling is to be believed, the word “suicide” has finally lost its shock value. Still, legislation continues to fail more often than it passes, even in blue states like Massachusetts and Connecticut. Right now, it’s just too early to tell.
Every story has an ending. This one, it turns out, hasn’t quite ended yet, but the beginning of the end came in 2014, when I too broke a bone. In my case, it was a bone in my back, and when I woke up on the morning of October 18, I couldn’t move. My wife called 911, and a few minutes later a crew of burly firefighters loaded me onto a stretcher and carried me downstairs to a waiting ambulance.

In the ER, the first thing they did was take a set of X-rays. A few hours later a doctor delivered the news in matter-of-fact tones: They had found lytic lesions on bones all over my body—on my legs, my skull, my hips, and my arms. Further tests were needed to confirm the ER doctor’s diagnosis, but there was really only one thing that could cause this. Like Harry, I had multiple myeloma.
That’s the bad news. The good news is that Mother Jones provides excellent health care coverage for its employees. I spent a week in the hospital, where I got a kyphoplasty to repair the bone and began the first stage of chemotherapy. After 16 weeks, the level of cancerous cells in my bone marrow had decreased from about 50 percent to 5 percent, good enough that I qualified for the second stage of treatment, an autologous stem cell transplant.
In concept, this is a simple procedure. First, I spent a couple of days having bone marrow stem cells extracted from my blood and then frozen. A couple of weeks later I was given a huge dose of a powerful chemotherapy drug that’s basically designed to kill everything in its path—including all my healthy bone marrow stem cells. This would kill me in short order, so the next day my stem cells were unfrozen and pumped back into my body. That’s it. All the rest was recovery. My immune system died off completely within a few days, and then started rebounding. After a couple of weeks I went home. Two months after that I felt fine.
Unfortunately, the procedure didn’t work. My bone marrow was still 5 percent cancerous. So now I’m on stage three, a different chemotherapy drug. It’s working, but it’s not working all that well. My last lab test showed that my bone marrow is only 4 percent cancerous, which is the right direction but not the right magnitude. There’s no known treatment that puts multiple myeloma in complete remission, but the goal is to get close enough to zero that the cancerous cells are undetectable. I’m nowhere near that yet.
I may still get there. And if my current medication doesn’t do the job, there are other things to try. Nonetheless, even though I feel fine, the grim fact is that I’m responding to the chemotherapy only modestly.
So how long do I have to live? Five years? Ten years? Two? No one knows. But I’m 57 years old, and death is no longer so far away that I never think about it. The odds are slim that I’ll ever collect a Social Security check.
That makes this story a very personal one. Sometime in the next few years the cancer will start to progress rapidly and there will be no more treatments to try. My bones will become more brittle and may break or accumulate microfractures. My immune system will deteriorate, making me vulnerable to opportunistic outside infections. I may suffer from hemorrhages or renal failure. My bones will stop retaining calcium, which will build up instead in my bloodstream. I may be in great pain—or I may not. Multiple myeloma can end in a lot of different ways. But one thing is sure: Once any of these symptoms start up, I’ll be dead within a few weeks or months.
Like Harry, though, I’ve never intended to let that happen. I have no interest in trying to tell other people what to do if they find themselves close to death, but my choice has always been clear: I don’t want to die in pain—or drugged into a stupor by pain meds—all while connected to tubes and respirators in a hospital room. When the end is near, I want to take my own life.
Until this year, that would have left me with only two options. The first is to wait until my wife is out of the house and lug out a helium tank. Assuming I do everything right, I’ll die quickly and painlessly—but I’ll also die alone. I would have no chance to say goodbye to friends and family, nor they to me. My wife would have the horror of discovering my corpse when she came home, and that would be her final memory of me.
The second option is that I’d wait too long and land in a hospital. I’d end up with all those tubes and pain meds I never wanted, and I’d never get out. Maybe I’d be there for a week, maybe a few months. Who knows? It’s pretty much my worst nightmare.

But now I have a third option. When I’m within six months of death, I can ask my doctor for a prescription sedative that will kill me on my own terms—when I want and where I want. Will I ever use it? I don’t know. I suspect that taking your own life requires a certain amount of courage, and I don’t know if I have it. Probably none of us do until we’re faced with it head-on.
But either way, I won’t have to die before I want to out of fear that I’ll lose the capacity to control my own destiny if I wait too long. Nor will I have to die alone out of fear that anyone present runs the risk of being hauled in by an overzealous sheriff’s deputy. I’ll be able to tell my wife I love her one last time. I can take her hand and we can lie down together on our bed. And then, slowly and peacefully, I’ll draw my last breaths.
I don’t want to die. But if I have to, this is how I want it to happen. I don’t want a “suicide party,” but neither do I want to suffer needlessly for months. Nor do I want to cause other people any more pain than I have to. I want to go out quietly, with my loved ones at my side.
When he signed California’s right-to-die bill, Gov. Brown attached a signing statement. “I do not know what I would do if I were dying in prolonged and excruciating pain,” he wrote. “I am certain, however, that it would be a comfort to be able to consider the options afforded by this bill. And I wouldn’t deny that right to others.”
Nor would I.