The graphic on the right won’t come as a surprise to anyone who’s read this blog over the years. It comes from the New York Times today, and it illustrates the fact that medical procedures cost  way, way more in the United States than in other countries. But why?
way, way more in the United States than in other countries. But why?
In the case of prescription drugs, the answer is supposedly that other countries are free riding off of us. If everyone paid $6 for Lipitor, then Pfizer never would have developed it in the first place. It wouldn’t have been worth it. It’s only the fact that Americans pay full market value for Lipitor that allows other countries to artificially force down the cost for their residents.
There may or may not be something to this, but at least it’s an explanation. What about MRI scans, though? MRI machines cost the same in the Netherlands as they do here, and they’re utilized just as heavily in both countries. So why the higher price in America? Some of the answer is in the cost of the personnel: we pay doctors and technicians more than most countries do, and that all goes into the price charged for diagnostic procedures. But does that explain a 4x price difference? Or the stunning 26x price difference in an angiogram between the U.S. and Canada?
Probably not. So Times reporter Elisabeth Rosenthal decided to dive into one particular procedure: colonoscopies. Why are they more expensive in the U.S. than elsewhere?
Largely an office procedure when widespread screening was first recommended, colonoscopies have moved into surgery centers — which were created as a step down from costly hospital care but are now often a lucrative step up from doctors’ examining rooms — where they are billed like a quasi operation. They are often prescribed and performed more frequently than medical guidelines recommend.
The high price paid for colonoscopies mostly results not from top-notch patient care, according to interviews with health care experts and economists, but from business plans seeking to maximize revenue; haggling between hospitals and insurers that have no relation to the actual costs of performing the procedure; and lobbying, marketing and turf battles among specialists that increase patient fees.
While several cheaper and less invasive tests to screen for colon cancer are recommended as equally effective by the federal government’s expert panel on preventive care — and are commonly used in other countries — colonoscopy has become the go-to procedure in the United States. “We’ve defaulted to by far the most expensive option, without much if any data to support it,” said Dr. H. Gilbert Welch, a professor of medicine at the Dartmouth Institute for Health Policy and Clinical Practice.
The “turf battles” mentioned above are about the routine use of anesthesiologists in colonoscopies, even though most aren’t done under a general anesthetic. This drives the price way up:
In Austria, where colonoscopies are also used widely for cancer screening, the procedure is performed, with sedation, in the office by a doctor and a nurse and “is very safe that way,” said Dr. Monika Ferlitsch, a gastroenterologist and professor at the Medical University of Vienna, who directs the national program on quality assurance.
….Dr. Cesare Hassan, an Italian gastroenterologist who is the chairman of the Guidelines Committee of the European Society of Gastrointestinal Endoscopy, noted that studies in Europe had estimated that the procedure cost about $400 to $800 to perform, including biopsies and sedation. “The U.S. is paying way too much for too little — it leads to opportunistic colonoscopies,” done for profit rather than health, he said.
Bottom line: if a colonoscopy is performed in a doctor’s office without an anesthesiologist, the price is cut in half—maybe more. Cut the number of colonoscopies and increase the use of other tests that are frequently just as good, and the average cost of colon cancer screening in America might drop by three-quarters.
But don’t expect this to happen anytime soon. After all, one man’s outrageous costs are another man’s Mercedes Benz. Welcome to the best health care in the world, baby.

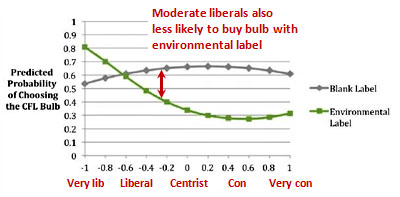 environmental message than when it was unlabeled.” But Tim Carney points out that
environmental message than when it was unlabeled.” But Tim Carney points out that 
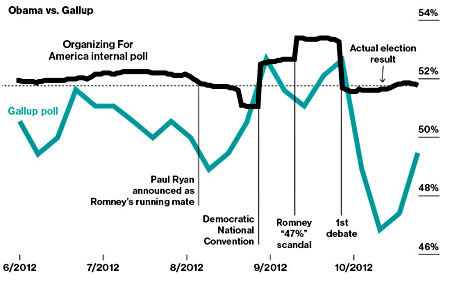 Pollster shows Romney gaining 2.4 points and RCP shows Romney gaining 1.8 points.”
Pollster shows Romney gaining 2.4 points and RCP shows Romney gaining 1.8 points.”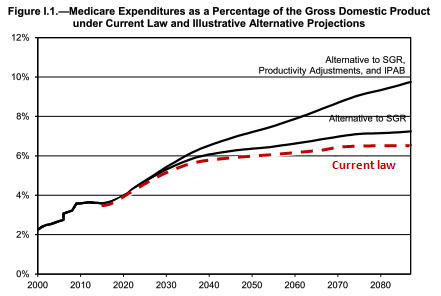 costs….and (iii) a refinement in projection methods that reduces assumed per beneficiary cost growth.
costs….and (iii) a refinement in projection methods that reduces assumed per beneficiary cost growth. breathlessly, “strongly suggests coordination by White House officials in the campaign against the president’s political opponents.”
breathlessly, “strongly suggests coordination by White House officials in the campaign against the president’s political opponents.”