“We started it,” Gawande told me flatly. He argued that health providers are at the root of the country’s staggering opioid epidemic. He didn’t blame the pharmaceutical companies — although there is good evidence that they played a large role — but instead focused on how views of pain began to shift in the 1990s, with doctors urged to take their patients’ suffering more seriously.
The medical profession certainly shares some of the blame for this, but I wouldn’t go as far at Gawande. I’m open to correction on this, but my understanding is that it was really the confluence of three different things:
Doctors. During the 70s and 80s, the medical profession began to get more serious about pain treatment. Several influential articles in medical journals argued that patients who were treated with opioids rarely became addicted, and this contributed to an increased willingness to prescribe them.
Parents. During the 80s and 90s, parents became more insistent about treating pain in their children for things like sprained ankes and broken bones. Instead of aspirin, they wanted Vicodin. This made everyone, doctors and patients alike, more comfortable about using opioids.
Big Pharma. Pharmaceutical companies never bothered promoting morphine because it’s cheap and earns them no money. But when patented opioids like Percocet and OxyContin came onto the market, pain suddenly became a big moneymaker. This required steady introductions of new products as old ones went off patent, and therefore much more aggressive marketing than in the past.
In 2001, this all came together when The Joint Commission, which accredits medical facilities, issued new guidelines on pain:
Pain should be assessed in all patients.
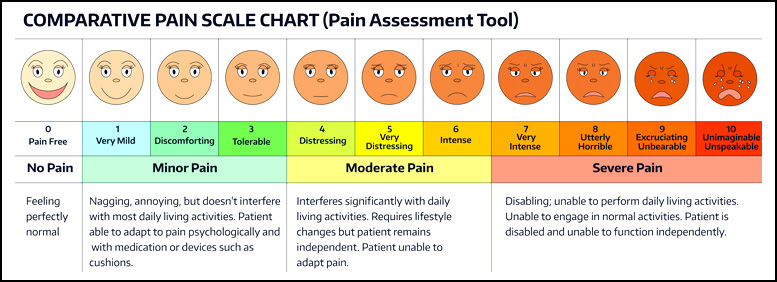
Pain intensity should be evaluated using the now-familiar 1-10 scale, and that scale should be prominently posted everywhere that patients are assessed.
Pain should be managed “aggressively and effectively.”
Patients should be instructed about pain and the importance of effective pain management.
These days, The Joint Commission is eager to disassociate itself from this mess. Last year they issued a statement saying that the 2001 standards never so much as mentioned opioids and certainly had nothing to do with rise in use of opioids. Needless to say, this is special pleading on steroids. It’s true that The Joint Commission didn’t start the opioid epidemic, but they certainly put their blessing on it. And there’s little question that both pharma and doctors lobbied for standards that mandated more aggressive pain management.
But that doesn’t let the rest of us off the hook. Boomer parents also bear some responsibility thanks to their unwillingness to tolerate even moderate pain in their children. Doctors were primed to respond, and even when they were skeptical they often decided that in the face of a demanding parent, the easiest course was just to prescribe an opioid and send everyone on their way. It’s not like the kids are all going to become junkies, right?
The goal now, obviously, is to substantially reduce the routine prescription of opioids for every ache and pain—especially in children and teens—but without making life hell for chronic pain sufferers who genuinely need strong medication. We need to react, but not overreact.
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?